OPSYNVI Film-coated tablet Ref.[109722] Active ingredients: Macitentan Macitentan and Tadalafil Tadalafil
Source: FDA, National Drug Code (US) Revision Year: 2024
12.1. Mechanism of Action
Macitentan
Endothelin (ET)-1 and its receptors (ETA and ETB) mediate a variety of deleterious effects, such as vasoconstriction, fibrosis, proliferation, hypertrophy, and inflammation. In disease conditions such as PAH, the local ET system is upregulated and is involved in vascular hypertrophy and in organ damage.
Macitentan is an endothelin receptor antagonist that inhibits the binding of ET-1 to both ETA and ETB receptors. Macitentan displays high affinity and sustained occupancy of the ET receptors in human pulmonary arterial smooth muscle cells. One of the metabolites of macitentan is also pharmacologically active at the ET receptors and is estimated to be about 20% as potent as the parent drug in vitro. The clinical impact of dual endothelin blockage is unknown.
Tadalafil
Tadalafil is an inhibitor of phosphodiesterase type 5 (PDE5), the enzyme responsible for the degradation of cyclic guanosine monophosphate (cGMP). PAH is associated with impaired release of nitric oxide by the vascular endothelium and consequent reduction of cGMP concentrations in the pulmonary vascular smooth muscle. PDE5 is the predominant phosphodiesterase in the pulmonary vasculature. Inhibition of PDE5 by tadalafil increases the concentrations of cGMP resulting in relaxation of pulmonary vascular smooth muscle cells and vasodilation of the pulmonary vascular bed.
Studies in vitro have shown that tadalafil is a selective inhibitor of PDE5. PDE5 is an enzyme found in corpus cavernosum, vascular smooth muscle, visceral smooth muscle, skeletal muscle, platelets, kidney, lung, and cerebellum. The effect of tadalafil is more potent on PDE5 than on other phosphodiesterases. Tadalafil is >10,000-fold more potent for PDE5 than for PDE1, PDE2, PDE4 and PDE7, enzymes which are found in the heart, brain, blood vessels, liver, and other organs. Tadalafil is >10,000-fold more potent for PDE5 than for PDE3, an enzyme found in the heart and blood vessels. This selectivity for PDE5 over PDE3 is important because PDE3 is an enzyme involved in cardiac contractility. Additionally, tadalafil is approximately 700-fold more potent for PDE5 than for PDE6, an enzyme which is found in the retina and is responsible for phototransduction. Tadalafil is also >9,000-fold more potent for PDE5 than for PDE8, PDE9 and PDE10.
12.2. Pharmacodynamics
Pharmacodynamic studies with OPSYNVI have not been conducted. As OPSYNVI contains macitentan and tadalafil, the pharmacodynamic effects for each component should be considered.
Pulmonary Hemodynamics of Macitentan
The SERAPHIN clinical efficacy study in patients with PAH assessed hemodynamic parameters in a subset of patients after 6 months of treatment. Patients treated with macitentan 10 mg (N=57) achieved a median reduction of 37% (95% CI 22–49) in pulmonary vascular resistance and an increase of 0.6 L/min/m2 (95% CI 0.3–0.9) in cardiac index compared to placebo (N=67).
Effects on Cardiac Electrophysiology
Macitentan
In a randomized, placebo-controlled four-way crossover study with a positive control in healthy subjects, repeated doses of macitentan 10 and 30 mg (3 times the recommended dosage) had no significant effect on the QTc interval.
Tadalafil
In a randomized, placebo-controlled four-way crossover study with a positive control in healthy subjects, a single dose of 100 mg tadalafil (2.5 times the recommended dosage) had no significant effect on the QTc interval.
Effects on Blood Pressure When Administered with Nitrates
In clinical pharmacology studies, tadalafil (5 to 20 mg) was shown to potentiate the hypotensive effect of nitrates. Do not use OPSYNVI in patients taking any form of nitrates [see Contraindications (4.3)].
A double–blind, placebo–controlled, crossover study in 150 male subjects at least 40 years of age (including subjects with diabetes mellitus and/or controlled hypertension) assessed the interaction between nitroglycerin and tadalafil. Subjects received daily doses of tadalafil 20 mg or matching placebo for 7 days and then were given a single dose of 0.4 mg sublingual nitroglycerin (NTG) at pre–specified timepoints following their last dose of tadalafil (2, 4, 8, 24, 48, 72, and 96 hours after tadalafil). A significant interaction between tadalafil and NTG was observed at each timepoint up to and including 24 hours. At 48 hours, by most hemodynamic measures, the interaction between tadalafil and NTG was not observed, although a few more tadalafil subjects compared to placebo experienced greater blood-pressure-lowering effects at this timepoint. After 48 hours, the interaction was not detectable [see Contraindications (4.3)].
Effects on Vision
Single oral doses of PDE inhibitors have demonstrated transient dose-related impairment of color discrimination (blue/green), using the Farnsworth–Munsell 100–hue test, with peak effects near the time of peak plasma levels. This finding is consistent with the inhibition of PDE6, which is involved in phototransduction in the retina. In a study to assess the effects of a single dose of tadalafil 40 mg on vision (N=59), no effects were observed on visual acuity, intraocular pressure, or pupillometry. Across all clinical studies with tadalafil, reports of changes in color vision were rare (<0.1% of patients).
Dose-Response Relationship
Dose-response relationships, between 20 mg and 40 mg of tadalafil, were not observed for 6-minute walk distance or pulmonary vascular resistance (PVR) in subjects with PAH in the placebo-controlled study. Median change from baseline in 6-minute walk distance was 32 meters and 35 meters at 16 weeks in subjects receiving 20 mg and 40 mg daily, respectively. Mean change from baseline PVR was -254 dynes*sec*cm and -209 dynes*sec*cm at 16 weeks in patients receiving 20 mg and 40 mg daily, respectively.
12.3. Pharmacokinetics
Macitentan
The pharmacokinetics of macitentan and its active metabolite have been studied primarily in healthy subjects. The pharmacokinetics of macitentan are dose proportional over a range from 1 mg to 30 mg after once daily administration.
A cross study comparison shows that the exposures to macitentan and its active metabolite in patients with PAH are similar to those observed in healthy subjects.
Tadalafil
Over a dose range of 2.5 to 20 mg, tadalafil exposure (AUC) increases proportionally with dose in healthy subjects. In PAH patients administered between 20 and 40 mg of tadalafil, an approximately 50% greater AUC was observed indicating a less than proportional increase in exposure over the entire dose range of 2.5 to 40 mg.
During tadalafil 20 and 40 mg once daily dosing, steady-state plasma concentrations were attained within 5 days, and exposure was approximately 30% higher than after a single dose.
Absorption
Macitentan
After a single oral administration of OPSYNVI, the maximum plasma concentration of macitentan is achieved in about 10 hours. The absolute bioavailability after oral administration is not known. In a study in healthy subjects, the exposure to macitentan and its active metabolite were unchanged after a high fat breakfast. OPSYNVI may therefore be taken with or without food.
Tadalafil
After a single oral-dose administration of OPSYNVI, the maximum observed plasma concentration (Cmax) of tadalafil is achieved in about 3 hours. Absolute bioavailability of tadalafil following oral dosing has not been determined. Food intake does not significantly alter the rate and extent of absorption of tadalafil and OPSYNVI may be taken with or without food.
Distribution
Macitentan
Macitentan and its active metabolite are highly bound to plasma proteins (>99%), primarily to albumin and to a lesser extent to alpha-1-acid glycoprotein. The apparent volumes of distribution (Vss/F) of macitentan and its active metabolite were about 50 L and 40 L respectively in healthy subjects.
Tadalafil
The mean apparent volume of distribution following oral administration is approximately 77 L, indicating that tadalafil is distributed into tissues. At therapeutic concentrations, 94% of tadalafil in plasma is bound to proteins.
Metabolism
Macitentan
Following oral administration, the apparent elimination half-lives of macitentan and its active metabolite are approximately 16 and 48 hours, respectively. Macitentan is metabolized primarily by oxidative depropylation of the sulfamide to form the pharmacologically active metabolite. This reaction is dependent on the cytochrome P450 (CYP) system, mainly CYP3A4 with minor contributions of CYP2C8, CYP2C9, and CYP2C19. At steady state in PAH patients, the systemic exposure to the active metabolite is 3-times the exposure to macitentan and is expected to contribute approximately 40% of the total pharmacologic activity.
Tadalafil
Tadalafil is predominantly metabolized by CYP3A to a catechol metabolite. The catechol metabolite undergoes extensive methylation and glucuronidation to form the methylcatechol and methylcatechol glucuronide conjugate, respectively. The major circulating metabolite is the methylcatechol glucuronide. Methylcatechol concentrations are less than 10% of glucuronide concentrations. In vitro data suggests that metabolites are not expected to be pharmacologically active at observed metabolite concentrations.
Elimination
Macitentan
In a study in healthy subjects with radiolabeled macitentan, approximately 50% of radioactive drug material was eliminated in urine but none was in the form of unchanged drug or the active metabolite. About 24% of the radioactive drug material was recovered from feces.
Tadalafil
Following 40 mg, the mean oral clearance for tadalafil is 3.4 L/hr and the mean effective half-life is 11 hours in healthy subjects. In patients with pulmonary hypertension not receiving concomitant bosentan, the mean oral clearance for tadalafil is 1.6 L/hr. Tadalafil is excreted predominantly as metabolites, mainly in the feces (approximately 61% of the dose) and to a lesser extent in the urine (approximately 36% of the dose).
Population Pharmacokinetics
Tadalafil
In patients with pulmonary hypertension not receiving concomitant bosentan, the average tadalafil exposure at steady-state following 40 mg was 26% higher when compared to those of healthy volunteers. The results suggest a lower clearance of tadalafil in patients with pulmonary hypertension compared to healthy volunteers.
Specific Populations
Renal Impairment
Macitentan:
Exposure to macitentan and its active metabolite in patients with severe renal impairment (creatinine clearance 15–29 mL/min) compared to healthy subjects was increased by 30% and 60%, respectively. This increase is not considered clinically relevant.
Tadalafil:
In clinical pharmacology studies using single-dose tadalafil (5 to 10 mg), tadalafil exposure (AUC) doubled in subjects with mild (creatinine clearance 51 to 80 mL/min) or moderate (creatinine clearance 30 to 50 mL/min) renal impairment. In subjects with end-stage renal disease on hemodialysis, Cmax doubled and AUC was 2.7 to 4.1 times as high following single-dose administration of 10 or 20 mg tadalafil, respectively. Exposure to total methylcatechol (unconjugated plus glucuronide) was 2 to 4-times as high in subjects with renal impairment, compared to those with normal renal function. Hemodialysis (performed between 24-and 30-hours post-dose) contributed negligibly to tadalafil or metabolite elimination.
Hepatic Impairment
Macitentan:
Exposure to macitentan was decreased by 21%, 34%, and 6% and exposure to the active metabolite was decreased by 20%, 25%, and 25% in subjects with mild, moderate, or severe hepatic impairment (Child-Pugh Class A, B, and C), respectively. This decrease is not considered clinically relevant.
Tadalafil:
In clinical pharmacology studies, tadalafil exposure (AUC) in subjects with mild or moderate hepatic impairment (Child-Pugh Class A or B) was similar to exposure in healthy subjects when a dose of 10 mg was administered. There are no available data for doses higher than 10 mg of tadalafil in patients with hepatic impairment. Insufficient data are available for subjects with severe hepatic impairment (Child-Pugh Class C) .
Geriatric Patients
Macitentan:
There are no clinically relevant effects of age on the pharmacokinetics of macitentan and its active metabolite.
Tadalafil:
In healthy male elderly subjects (65 years or over) after a 10 mg dose, a lower oral clearance of tadalafil, resulting in 25% higher exposure (AUC) with no effect on Cmax was observed relative to that in healthy subjects 19 to 45 years of age.
Patients with Diabetes Mellitus
Tadalafil:
In male patients with diabetes mellitus after a 10 mg tadalafil dose, exposure (AUC) was reduced approximately 19% and Cmax was 5% lower than that observed in healthy subjects. No dose adjustment is warranted.
Race and gender:
There are no clinically relevant effects of race or gender on macitentan, its active metabolite, or tadalafil.
Drug Interactions
No clinical study evaluating drug interactions has been performed using OPSYNVI. Interactions that have been identified in studies with individual components of OPSYNVI (macitentan or tadalafil) determine the interactions that may occur with OPSYNVI. Co-administration of macitentan (10 mg once daily) and tadalafil (40 mg once daily) had no clinically relevant effect on the pharmacokinetics of either macitentan or tadalafil.
Macitentan
The metabolism of macitentan to its active metabolite is catalyzed mainly by CYP3A4, with minor contributions from CYP2C8, CYP2C9, and CYP2C19.
Macitentan and its active metabolite do not have relevant inhibitory or inducing effects on CYP enzymes.
Macitentan and its active metabolite are not substrates of the multi-drug resistance protein (P-gp, MDR-1) or organic anion transporting polypeptides (OATP1B1 and OATP1B3).
Macitentan and its active metabolite are not inhibitors of hepatic or renal drug transporters at clinically relevant concentrations.
Tadalafil
Tadalafil is a substrate of and predominantly metabolized by CYP3A.
Effects of other drugs on macitentan or tadalafil
Strong CYP3A4 inducers or inhibitors
Macitentan:
Concomitant treatment with rifampicin 600 mg daily, a potent inducer of CYP3A4, reduced the steady-state exposure to macitentan by 79% but did not affect the exposure to the active metabolite [see Drug Interactions (7.2)].
Concomitant use of strong CYP3A4 inhibitors like ketoconazole approximately double macitentan exposure. Effects of other strong CYP3A4 inhibitors such as ritonavir on macitentan were not studied but are likely to result in an increase in macitentan exposure at steady state similar to that seen with ketoconazole [see Drug Interactions (7.3)].
A moderate dual inhibitor of CYP3A4 and CYP2C9 such as fluconazole (400 mg once daily) is predicted to increase macitentan exposure approximately 4-fold without relevant effect on the exposure to its active metabolite [see Drug Interactions (7.4)].
Tadalafil:
Rifampin (600 mg daily), a CYP3A inducer, reduced tadalafil 10 mg single-dose exposure (AUC) by 88% and Cmax by 46%, relative to the values for tadalafil 10 mg alone [see Drug Interactions (7.2)].
Bosentan, a substrate of CYP2C9 and CYP3A and a moderate inducer of CYP3A, CYP2C9 and possibly CYP2C19, reduced tadalafil systemic exposure following multiple-dose coadministration. Although specific interactions have not been studied, other CYP3A inducers, such as carbamazepine, phenytoin, and phenobarbital, would likely decrease tadalafil exposure [see Drug Interactions (7.2)].
Ketoconazole increased tadalafil exposure relative to the values for tadalafil alone. Although specific interactions have not been studied, other CYP3A inhibitors, such as erythromycin, itraconazole, and grapefruit juice, would likely increase tadalafil exposure [see Drug Interactions (7.3)].
Ritonavir increased tadalafil 20-mg single-dose exposure relative to the values for tadalafil alone. Ritonavir inhibits and induces CYP3A, the enzyme involved in the metabolism of tadalafil, in a time-dependent manner. The initial inhibitory effect of ritonavir on CYP3A may be mitigated by a more slowly evolving induction effect so that after about 1 week of ritonavir twice daily, the exposure of tadalafil is similar in the presence of and absence of ritonavir [see Drug Interactions (7.3)].
Effects of macitentan or tadalafil on other medicinal products
Macitentan
Macitentan once daily dosing did not alter the exposure to R- and S-warfarin or their effect on international normalized ratio (INR).
At steady state, the exposure to sildenafil 20 mg t.i.d. increased by 15% during concomitant administration of macitentan 10 mg once daily. This change is not considered clinically relevant. Macitentan 10 mg once daily did not affect the pharmacokinetics of an oral contraceptive (norethisterone 1 mg and ethinyl estradiol 35 µg).
Macitentan 10 mg once daily did not affect the pharmacokinetics of concomitant use of a BCRP substrate drug (riociguat 1 mg and rosuvastatin 10 mg).
Tadalafil
Tadalafil is not expected to cause clinically significant inhibition or induction of the clearance of drugs metabolized by cytochrome P450 (CYP) isoforms.
Exposure changes of drugs following co-administration with tadalafil are shown in Figure 1.
Figure 1. Impact of Tadalafil on the Pharmacokinetics of Other Drugs:

a A small augmentation (increase of 3 beats per minute) in heart rate was observed with theophylline.
b Tadalafil (40 mg qd) had no clinically significant effect on exposure (AUC and C) of bosentan metabolites.
c 95% CI
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Macitentan
Carcinogenicity studies of 2 years' duration did not reveal any carcinogenic potential at exposures 75-fold and 140-fold the human exposure (based on AUC) in male and female mice, respectively, and 8.3-and 42-fold in male and female rats, respectively.
Tadalafil
Tadalafil was not carcinogenic to rats or mice when administered daily for 2 years at doses up to 400 mg/kg/day. Systemic drug exposures, as measured by AUC of unbound tadalafil, were approximately 5-fold for mice, and 7-and 14-fold for male and female rats, respectively, the exposures at the maximum recommended human dose (MRHD) of 40 mg.
Mutagenesis
Macitentan
Macitentan was not genotoxic in a standard battery of in vitro and in vivo assays that included a bacterial reverse mutation assay, an assay for gene mutations in mouse lymphoma cells, a chromosome aberration test in human lymphocytes, and an in vivo micronucleus test in rats.
Tadalafil
Tadalafil was not mutagenic in the in vitro bacterial Ames assays or the forward mutation test in mouse lymphoma cells. Tadalafil was not clastogenic in the in vitro chromosomal aberration test in human lymphocytes or the in vivo rat micronucleus assays.
Impairment of Fertility
Macitentan
Treatment of juvenile rats from postnatal Day 4 to Day 114 led to reduced body weight gain and testicular tubular atrophy at exposures 7-fold the human exposure. Fertility was not affected.
Reversible testicular tubular dilatation was observed in chronic toxicity studies at exposures greater than 7-fold and 23-fold the human exposure in rats and dogs, respectively. After 2 years of treatment, tubular atrophy was seen in rats at 4-fold the human exposure. Macitentan did not affect male or female fertility at exposures ranging from 19-to 44-fold the human exposure, respectively, and had no effect on sperm count, motility, and morphology in male rats. No testicular findings were noted in mice after treatment up to 2 years.
Tadalafil
There were no effects on fertility, reproductive performance or reproductive organ morphology in male or female rats given oral doses of tadalafil up to 400 mg/kg/day, a dose producing AUCs for unbound tadalafil of 6-fold for males or 17-fold for females the exposures at the MRHD of 40 mg. In beagle dogs given tadalafil daily for 3 to 12 months, there was treatment-related non-reversible degeneration and atrophy of the seminiferous tubular epithelium in the testes in 20–100% of the dogs that resulted in a decrease in spermatogenesis in 40–75% of the dogs at doses of ≥10 mg/kg/day. Systemic exposure (based on AUC) at no-observed-adverse-effect-level (NOAEL) (10 mg/kg/day) for unbound tadalafil was similar to that expected in humans at the MRHD of 40 mg.
There were no treatment-related testicular findings in rats or mice treated with doses up to 400 mg/kg/day for 2 years.
13.2. Animal Toxicology and/or Pharmacology
Macitentan
In dogs, macitentan decreased blood pressure at exposures similar to the therapeutic human exposure. Intimal thickening of coronary arteries was observed at 17-fold the human exposure after 4 to 39 weeks of treatment. Due to the species-specific sensitivity and the safety margin, this finding is considered not relevant for humans.
There were no adverse liver findings in long-term studies conducted in mice, rats and dogs at exposures of 12-to 116-fold the human exposure.
Tadalafil
Animal studies showed vascular inflammation in tadalafil-treated mice, rats, and dogs. In mice and rats, lymphoid necrosis and hemorrhage were seen in the spleen, thymus, and mesenteric lymph nodes at unbound tadalafil exposure of 1-to 17-fold the human exposure (AUCs) at the MRHD of 40 mg. In dogs, an increased incidence of disseminated arteritis was observed in 1-and 6-month studies at unbound tadalafil exposure of 0.5-to 38-fold the human exposure (AUC) at the MRHD of 40 mg. In a 12-month dog study, no disseminated arteritis was observed, but 2 dogs exhibited marked decreases in white blood cells (neutrophils) and moderate decreases in platelets with inflammatory signs at unbound tadalafil exposures of approximately 4-to 10-fold the human exposure at the MRHD of 40 mg. The abnormal blood-cell findings were reversible within 2 weeks upon removal of the drug.
14. Clinical Studies
14.1 Pulmonary Arterial Hypertension
OPSYNVI
OPSYNVI was demonstrated to reduce pulmonary vascular resistance (PVR) in a multi-national, multi-center, double-blind, adaptive, randomized, active-controlled, parallel-group study [NCT03904693 (A DUE)] in 187 patients with PAH (WHO FC II–III). The study was designed to compare the efficacy and safety of OPSYNVI to each monotherapy macitentan or tadalafil. Patients with PVR of at least 240 dyn∙s/cm5 were randomized to receive OPSYNVI (n=108), 10 mg macitentan monotherapy (n=35) or 40 mg tadalafil monotherapy (n=44), once daily.
Patients who received treatment during the double-blind treatment period (n=186) were either treatment-naïve (53%) or on an ERA (17%) or a PDE5 inhibitor (30%). Patients enrolled had idiopathic PAH (51%), heritable PAH (5%), PAH associated with connective tissue disease (35%), or PAH associated with congenital heart disease (3%). The mean age was 50 years (range 18–80), 20% of patients were ≥65 years of age, 22% were male and 62% were white. At the time of enrollment, 51% of patients were WHO FC II and 49% were WHO FC III.
Patients who were not on a therapeutic PDE5 inhibitor dose at baseline received a 1-week titration period of macitentan 10 mg and tadalafil 20 mg.
The primary endpoint of the study was change from baseline in PVR (expressed as the ratio of geometric means of end of double-blind treatment to baseline) vs the individual component monotherapies after 16 weeks.
Hemodynamic
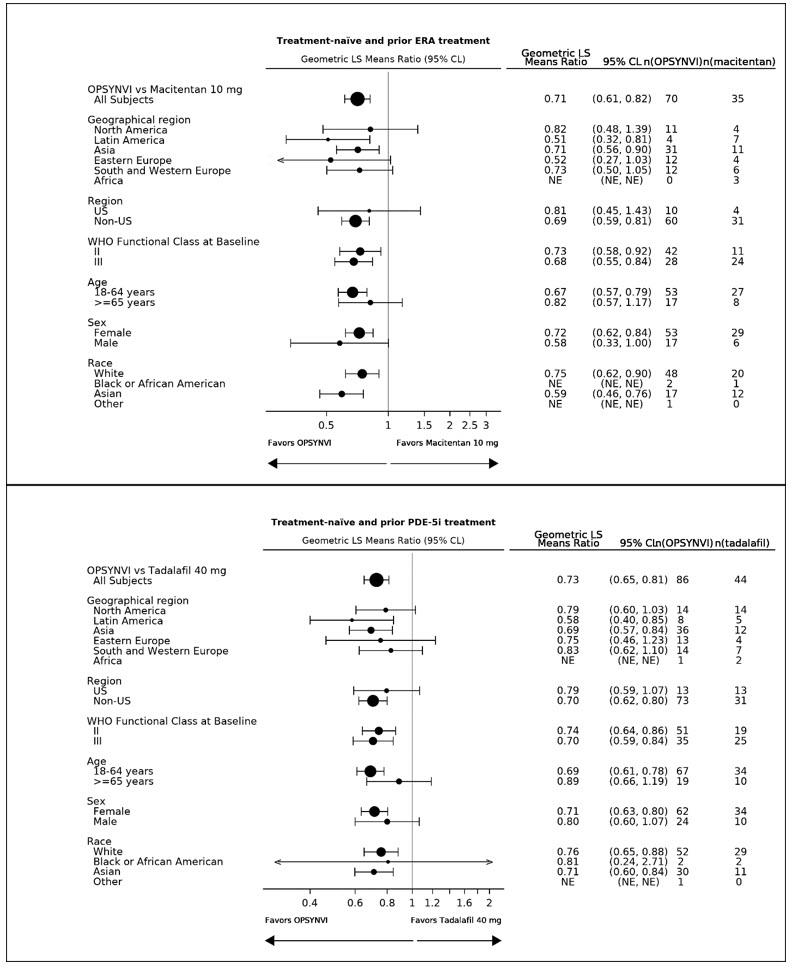
OPSYNVI demonstrated greater reduction in PVR after 16 weeks. Treatment with OPSYNVI resulted in a statistically significant treatment effect of 0.71 (95% CL 0.61, 0.82, p<0.0001) representing a 29% reduction in PVR as compared to macitentan, and of 0.72 (95% CLs 0.64, 0.80, p<0.0001) representing a 28% reduction in PVR as compared to tadalafil (Table 4).
Table 4. Change from Baseline in PVR at Week 16*:
| Treatment-naïve and Prior ERA Treatment | Treatment-naïve and Prior PDE5 Inhibitor Treatment | |||
|---|---|---|---|---|
| Macitentan (n=35) | OPSYNVI (n=70) | Tadalafil (n=44) | OPSYNVI (n=86) | |
| Baseline mean (SD) | 816 (401) | 834 (631) | 802 (552) | 885(640) |
| Reduction at Week 16 (dynes *sec/cm5) Mean (SD) | -162 (240) | -371 (429) | -181 (238) | -385 (396) |
| Geometric mean (Week 16/Baseline) | 0.77 | 0.55 | 0.78 | 0.56 |
| Treatment effect ratios (95% CL) | -29% (-39%, -18%) | -28% (-36%, -20%) | ||
| 2-sided p-value | <0.0001 | <0.0001 | ||
A consistent effect of OPSYNVI on reducing PVR was seen across subgroups of age, sex, race, geographical region, and baseline WHO FC (see Figure 2). Additionally, a consistent effect was observed in patients who were either treatment-naïve, or previously exposed to an ERA or PDE5 inhibitor.
Figure 2. Subgroup Analysis of the A DUE Study:
The individual components of OPSYNVI, macitentan and tadalafil, have been approved and used independently or concomitantly in the clinical setting to effectively manage PAH. Macitentan is an endothelin receptor antagonist (ERA) indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to reduce the risks of disease progression and hospitalization for PAH. Tadalafil is a phosphodiesterase 5 (PDE5) inhibitor indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group 1) to improve exercise ability.
Macitentan
The primary efficacy endpoint of the multi-center, long-term, placebo-controlled SERAPHIN study was time to the first occurrence of death, a significant morbidity event, defined as atrial septostomy, lung transplantation, initiation of intravenous or subcutaneous prostanoids, or “other worsening of PAH” during double-blind treatment plus 7 days. Other worsening was defined as all of the following: 1) a sustained ≥15% decrease from baseline in 6-minute walk distance (6MWD), 2) worsening of PAH symptoms (worsening of WHO FC), and 3) need for additional treatment for PAH. All of these other worsening events were confirmed by an independent adjudication committee, blinded to treatment allocation.
Treatment with OPSUMIT 10 mg reduced the risk of clinical worsening events and hospitalization for PAH.
Tadalafil
The primary efficacy endpoint of a randomized, 16-week placebo-controlled study was the change from baseline at week 16 in 6-minute walk distance. Treatment with tadalafil 40 mg improved exercise ability.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.