ABSORICA Capsule Ref.[50736] Active ingredients: Isotretinoin
Source: FDA, National Drug Code (US) Revision Year: 2022
12.1. Mechanism of Action
ABSORICA/ABSORICA LD is a retinoid, which when administered at the recommended dosage [see Dosage and Administration (2.1)], inhibits sebaceous gland function and keratinization. Clinical improvement in nodular acne patients occurs in association with a reduction in sebum secretion. The decrease in sebum secretion is temporary and is related to the dose and duration of treatment with isotretinoin capsules and reflects a reduction in sebaceous gland size and an inhibition of sebaceous gland differentiation. The exact mechanism of action of ABSORICA/ABSORICA LD in the treatment of severe recalcitrant nodular acne is unknown.
12.2. Pharmacodynamics
The pharmacodynamics of ABSORICA/ABSORICA LD are unknown.
12.3. Pharmacokinetics
No clinically significant differences in the pharmacokinetics of isotretinoin between patients with nodular acne and healthy subjects without acne were reported in published literature.
Absorption Following ABSORICA Administration
The ABSORICA mean Tmax was 6.4 hours under fed conditions and 2.9 hours under fasting conditions following administration of a single 40 mg dose.
Effect on Food
No clinically significant differences in ABSORICA pharmacokinetics were observed following administration with a modified high-fat, high-calorie meal (123.2 calories from protein, 265.6 calories from carbohydrates, and 468 calories from fat; total calories 857 calories) with reduced vitamin A content. The mean AUC0-t and Cmax of isotretinoin were 6095 ng*hr/mL and 369 ng/mL, respectively, following administration of a single 40 mg ABSORICA dose under fed conditions; which were approximately 50% and 26% higher, respectively, compared to fasting conditions. However, ABSORICA may be given with or without meals [see Dosage and Administration (2.1)].
Absorption Following ABSORICA LD Administration
The ABSORICA LD median Tmax was 5 hours under fed conditions and 3.5 hours under fasting conditions following administration of a single 32 mg dose.
Effect on Food<
No clinically significant differences in ABSORICA LD pharmacokinetics were observed following administration with a high-fat, high-calorie meal (150 calories from protein, 250 calories from carbohydrates, and 500 calories from fat; total calories 900 calories). The mean AUC0-t and Cmax of isotretinoin were 10209 ng*hr/mL and 646 ng/mL, respectively, following administration of a single 32 mg ABSORICA LD dose under fed conditions; which were approximately 20% and 6% higher, respectively, compared to fasting conditions. However, ABSORICA LD may be given with or without meals [see Dosage and Administration (2.1)].
Distribution
Isotretinoin is more than 99.9% bound to plasma proteins, primarily albumin.
Elimination
The mean elimination half-lives of isotretinoin and its 4-oxo-isotretinoin metabolite were:
- 18 hours and 38 hours, respectively, after a single oral ABSORICA 40 mg dose.
- Approximately 24 hours and 38 hours, respectively, after a single oral ABSORICA LD 32 mg dose.
Metabolism
Isotretinoin is primarily metabolized by CYP2C8, 2C9, 3A4, and 2B6 in vitro. Isotretinoin and its metabolites are further metabolized into conjugates.
Following oral administration of isotretinoin capsules, at least three metabolites (4-oxo-isotretinoin, retinoic acid (tretinoin), and 4-oxo-retinoic acid (4-oxo-tretinoin)) have been identified in human plasma. The extent of formation of all metabolites was higher under fed conditions. All of these metabolites possess retinoid activity in vitro. The clinical significance is unknown.
Excretion
Following oral administration of an 80 mg dose of radiolabeled-isotretinoin as a liquid suspension, the metabolites of isotretinoin were excreted in feces and urine in relatively equal amounts (total of 65% to 83%).
Specific Populations
Pediatric Patients: No clinically significant differences in the pharmacokinetics of isotretinoin were observed based on age (12 to 15 years (n=38), and ≥18 years (n=19)). In both age groups, 4-oxo-isotretinoin was the major metabolite; tretinoin and 4-oxo-tretinoin were also observed [see Use in Specific Populations (8.4)].
Drug Interaction Studies
No clinically significant differences in the pharmacokinetics of phenytoin (CYP2C9 substrate) were observed when used concomitantly with isotretinoin.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
In male and female Fischer 344 rats given oral isotretinoin at dosages of 8 or 32 mg/kg/day (1.3 or 5.3 times the recommended clinical ABSORICA dosage of 1 mg/kg/day or the recommended clinical ABSORICA LD dosage of 0.8 mg/kg/day, respectively, after normalization for total body surface area) for greater than 18 months, there was a dose-related increased incidence of pheochromocytoma relative to controls. The incidence of adrenal medullary hyperplasia was also increased at the higher dosage in both sexes. The relatively high level of spontaneous pheochromocytomas occurring in the male Fischer 344 rat makes it an equivocal model for study of this tumor; therefore, the relevance of this tumor to humans is uncertain.
The Ames test was conducted with isotretinoin in two laboratories. The results of the tests in one laboratory were negative, while in the second laboratory, a weakly positive response (less than 1.6 times background) was noted in S. typhimurium TA100 when the assay was conducted with metabolic activation. No dose response effect was seen, and all other strains were negative. Additionally, other tests designed to assess genotoxicity (Chinese hamster cell assay, mouse micronucleus test, S. cerevisiae D7 assay, in vitro clastogenesis assay with human-derived lymphocytes, and unscheduled DNA synthesis assay) were all negative.
In rats, no adverse effects on gonadal function, fertility, conception rate, gestation or parturition were observed at oral dosages of isotretinoin of 2, 8, or 32 mg/kg/day (0.3, 1.3, or 5.3 times the recommended clinical ABSORICA dosage of 1 mg/kg/day or the recommended clinical ABSORICA LD dosage of 0.8 mg/kg/day, respectively, after normalization for total body surface area).
In dogs, testicular atrophy was noted after treatment with oral isotretinoin for approximately 30 weeks at dosages of 20 or 60 mg/kg/day (10 or 30 times the recommended clinical ABSORICA dosage of 1 mg/kg/day or the recommended clinical ABSORICA LD dosage of 0.8 mg/kg/day, respectively, after normalization for total body surface area). In general, there was microscopic evidence for appreciable depression of spermatogenesis, but some sperm were observed in all testes examined, and in no instance were completely atrophic tubules seen.
13.2. Animal Toxicology and/or Pharmacology
In rats given 8 or 32 mg/kg/day of isotretinoin (1.3 or 5.3 times the recommended clinical ABSORICA dosage of 1 mg/kg/day or the recommended clinical ABSORICA LD dosage of 0.8 mg/kg/day, respectively, after normalization for total body surface area) for 18 months or longer, the incidences of focal calcification, fibrosis and inflammation of the myocardium, calcification of coronary, pulmonary and mesenteric arteries, and metastatic calcification of the gastric mucosa were greater than in control rats of similar age. Focal endocardial and myocardial calcifications associated with calcification of the coronary arteries were observed in two dogs after approximately 6 to 7 months of treatment with isotretinoin at a dosage of 60 to 120 mg/kg/day (30 to 60 times the recommended clinical ABSORICA dosage of 1 mg/kg/day or the recommended clinical ABSORICA LD dosage of 0.8 mg/kg/day, respectively, after normalization for total body surface area).
14. Clinical Studies
The effectiveness of ABSORICA/ABSORICA LD for the treatment of severe recalcitrant nodular acne in patients 12 years of age and older has been established and is based on a double-blind, randomized, parallel group trial (Study 1) in subjects with severe recalcitrant nodular acne who received ABSORICA or another isotretinoin capsule product under fed conditions. A total of 925 subjects were randomized 1:1 to receive ABSORICA or another isotretinoin capsule product. Study subjects ranged from 12 to 54 years of age (including 397 pediatric subjects 12 to 17 years old); 60% were male, 40% were female; and the racial groups included 87% White, 4% Black, 6% Asian, and 3% Other. Enrolled subjects had a weight of 40 to 110 kg and had at least 10 nodular lesions on the face and/or trunk. Subjects were treated with an initial dose of 0.5 mg/kg/day in two divided doses for the first 4 weeks, followed by 1 mg/kg/day in two divided doses for the following 16 weeks.
Change from baseline to Week 20 in total nodular lesion count and proportion of subjects with at least a 90% reduction in total nodular lesion count from baseline to Week 20 are presented in Table 3. Total nodular lesion counts by visit are presented in Figure 1. A single course of ABSORICA and another isotretinoin capsule product therapy for 15 to 20 weeks has been shown to result in complete and prolonged remission of acne in many patients.
Table 3. Efficacy Results in Subjects with Severe Recalcitrant Nodular Acne at Week 20 (Study 1):
| ABSORICA N=464 | Another Isotretinoin Capsule Product* N=461 | |
|---|---|---|
| Nodular Lesions Mean Baseline Count Mean Reduction | 18.4-15.68 | 17.7-15.62 |
| Subjects Achieving 90% Reduction, n (%) | 324 (70%) | 344 (75%) |
Figure 1. Total Nodular (Facial and Truncal) Lesion Count in Subjects with Severe Recalcitrant Nodular Acne by Visit in Study 1:
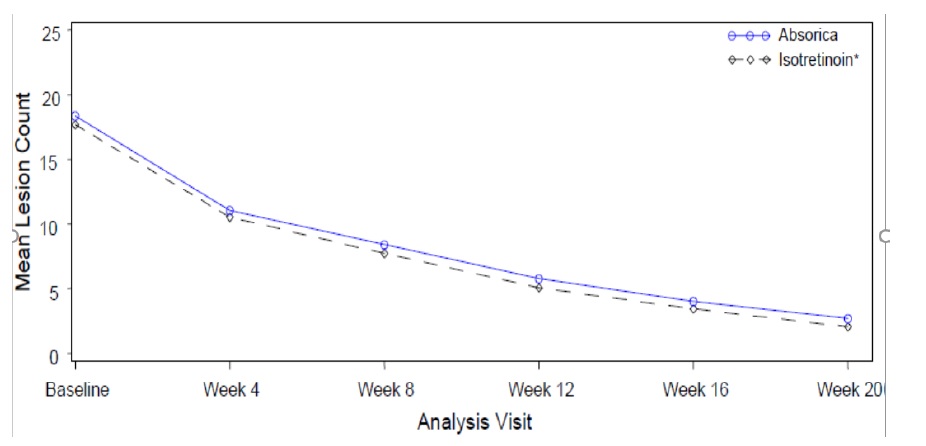
* Another isotretinoin capsule product.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.