CARVEDILOL Film-coated tablet Ref.[51669] Active ingredients: Carvedilol
Source: FDA, National Drug Code (US) Revision Year: 2023
12. Clinical Pharmacology
12.4 Specific Populations
Heart Failure
Steady-state plasma concentrations of carvedilol and its enantiomers increased proportionally over the 6.25- to 50- mg dose range in subjects with heart failure. Compared with healthy subjects, subjects with heart failure had increased mean AUC and Cmax values for carvedilol and its enantiomers, with up to 50% to 100% higher values observed in 6 subjects with NYHA class IV heart failure. The mean apparent terminal elimination half-life for carvedilol was similar to that observed in healthy subjects.
Geriatric
Plasma levels of carvedilol average about 50% higher in the elderly compared with young subjects.
Hepatic Impairment
Compared with healthy subjects, patients with severe liver impairment (cirrhosis) exhibit a 4- to 7-fold increase in carvedilol levels. Carvedilol is contraindicated in patients with severe liver impairment.
Renal Impairment
Although carvedilol is metabolized primarily by the liver, plasma concentrations of carvedilol have been reported to be increased in patients with renal impairment. Based on mean AUC data, approximately 40% to 50% higher plasma concentrations of carvedilol were observed in subjects with hypertension and moderate to severe renal impairment compared with a control group of subjects with hypertension and normal renal function. However, the ranges of AUC values were similar for both groups. Changes in mean peak plasma levels were less pronounced, approximately 12% to 26% higher in subjects with impaired renal function.
Consistent with its high degree of plasma protein-binding, carvedilol does not appear to be cleared significantly by hemodialysis.
12.5 Drug-Drug Interactions
Since carvedilol undergoes substantial oxidative metabolism, the metabolism and pharmacokinetics of carvedilol may be affected by induction or inhibition of cytochrome P450 enzymes.
Amiodarone
In a pharmacokinetic trial conducted in 106 Japanese subjects with heart failure, coadministration of small loading and maintenance doses of amiodarone with carvedilol resulted in at least a 2-fold increase in the steady-state trough concentrations of S(-)-carvedilol [see Drug Interactions (7.6)].
Cimetidine
In a pharmacokinetic trial conducted in 10 healthy male subjects, cimetidine (1,000 mg per day) increased the steady-state AUC of carvedilol by 30% with no change in Cmax [see Drug Interactions (7.5)].
Digoxin
Following concomitant administration of carvedilol (25 mg once daily) and digoxin (0.25 mg once daily) for 14 days, steady-state AUC and trough concentrations of digoxin were increased by 14% and 16%, respectively, in 12 subjects with hypertension [see Drug Interactions (7.4)].
Glyburide
In 12 healthy subjects, combined administration of carvedilol (25 mg once daily) and a single dose of glyburide did not result in a clinically relevant pharmacokinetic interaction for either compound.
Hydrochlorothiazide
A single oral dose of carvedilol 25 mg did not alter the pharmacokinetics of a single oral dose of hydrochlorothiazide 25 mg in 12 subjects with hypertension. Likewise, hydrochlorothiazide had no effect on the pharmacokinetics of carvedilol.
Rifampin
In a pharmacokinetic trial conducted in 8 healthy male subjects, rifampin (600 mg daily for 12 days) decreased the AUC and Cmax of carvedilol by about 70% [see Drug Interactions (7.5)].
Torsemide
In a trial of 12 healthy subjects, combined oral administration of carvedilol 25 mg once daily and torsemide 5 mg once daily for 5 days did not result in any significant differences in their pharmacokinetics compared with administration of the drugs alone.
Warfarin
Carvedilol (12.5 mg twice daily) did not have an effect on the steady-state prothrombin time ratios and did not alter the pharmacokinetics of R(+)- and S(-)-warfarin following concomitant administration with warfarin in 9 healthy volunteers.
12.1. Mechanism of Action
Carvedilol is a racemic mixture in which nonselective β-adrenoreceptor blocking activity is present in the S() enantiomer and α1-adrenergic blocking activity is present in both R(+) and S() enantiomers at equal potency. Carvedilol has no intrinsic sympathomimetic activity.
12.2. Pharmacodynamics
Heart Failure
The basis for the beneficial effects of carvedilol in heart failure is not established.
Two placebo-controlled trials compared the acute hemodynamic effects of carvedilol with baseline measurements in 59 and 49 subjects with NYHA class II to IV heart failure receiving diuretics, ACE inhibitors, and digitalis. There were significant reductions in systemic blood pressure, pulmonary artery pressure, pulmonary capillary wedge pressure, and heart rate. Initial effects on cardiac output, stroke volume index, and systemic vascular resistance were small and variable.
These trials measured hemodynamic effects again at 12 to 14 weeks. Carvedilol significantly reduced systemic blood pressure, pulmonary artery pressure, right atrial pressure, systemic vascular resistance, and heart rate, while stroke volume index was increased.
Among 839 subjects with NYHA class II to III heart failure treated for 26 to 52 weeks in 4 U.S. placebo-controlled trials, average left ventricular ejection fraction (EF) measured by radionuclide ventriculography increased by 9 EF units (%) in subjects receiving carvedilol and by 2 EF units in placebo subjects at a target dose of 25 to 50 mg twice daily. The effects of carvedilol on ejection fraction were related to dose. Doses of 6.25 mg twice daily, 12.5 mg twice daily, and 25 mg twice daily were associated with placebo-corrected increases in EF of 5 EF units, 6 EF units, and 8 EF units, respectively; each of these effects were nominally statistically significant.
Left Ventricular Dysfunction following Myocardial Infarction
The basis for the beneficial effects of carvedilol in patients with left ventricular dysfunction following an acute myocardial infarction is not established.
Hypertension
The mechanism by which β-blockade produces an antihypertensive effect has not been established.
β-adrenoreceptor blocking activity has been demonstrated in animal and human studies showing that carvedilol (1) reduces cardiac output in normal subjects, (2) reduces exercise- and/or isoproterenol-induced tachycardia, and (3) reduces reflex orthostatic tachycardia. Significant β-adrenoreceptor blocking effect is usually seen within 1 hour of drug administration.
α1-adrenoreceptor blocking activity has been demonstrated in human and animal studies, showing that carvedilol (1) attenuates the pressor effects of phenylephrine, (2) causes vasodilation, and (3) reduces peripheral vascular resistance. These effects contribute to the reduction of blood pressure and usually are seen within 30 minutes of drug administration.
Due to the α1-receptor blocking activity of carvedilol, blood pressure is lowered more in the standing than in the supine position, and symptoms of postural hypotension (1.8%), including rare instances of syncope, can occur. Following oral administration, when postural hypotension has occurred, it has been transient and is uncommon when carvedilol is administered with food at the recommended starting dose and titration increments are closely followed [see Dosage and Administration (2)].
In hypertensive patients with normal renal function, therapeutic doses of carvedilol decreased renal vascular resistance with no change in glomerular filtration rate or renal plasma flow. Changes in excretion of sodium, potassium, uric acid, and phosphorus in hypertensive patients with normal renal function were similar after carvedilol and placebo.
Carvedilol has little effect on plasma catecholamines, plasma aldosterone, or electrolyte levels, but it does significantly reduce plasma renin activity when given for at least 4 weeks. It also increases levels of atrial natriuretic peptide.
12.3. Pharmacokinetics
Carvedilol is rapidly and extensively absorbed following oral administration, with absolute bioavailability of approximately 25% to 35% due to a significant degree of first-pass metabolism. Following oral administration, the apparent mean terminal elimination half-life of carvedilol generally ranges from 7 to 10 hours. Plasma concentrations achieved are proportional to the oral dose administered. When administered with food, the rate of absorption is slowed, as evidenced by a delay in the time to reach peak plasma levels, with no significant difference in extent of bioavailability. Taking carvedilol with food should minimize the risk of orthostatic hypotension.
Carvedilol is extensively metabolized. Following oral administration of radiolabelled carvedilol to healthy volunteers, carvedilol accounted for only about 7% of the total radioactivity in plasma as measured by area under the curve (AUC). Less than 2% of the dose was excreted unchanged in the urine. Carvedilol is metabolized primarily by aromatic ring oxidation and glucuronidation. The oxidative metabolites are further metabolized by conjugation via glucuronidation and sulfation. The metabolites of carvedilol are excreted primarily via the bile into the feces. Demethylation and hydroxylation at the phenol ring produce 3 active metabolites with β-receptor blocking activity. Based on preclinical studies, the 4'-hydroxyphenyl metabolite is approximately 13 times more potent than carvedilol for β-blockade.
Compared with carvedilol, the 3 active metabolites exhibit weak vasodilating activity. Plasma concentrations of the active metabolites are about one-tenth of those observed for carvedilol and have pharmacokinetics similar to the parent.
Carvedilol undergoes stereoselective first-pass metabolism with plasma levels of R( + )-carvedilol approximately 2 to 3 times higher than S( - )-carvedilol following oral administration in healthy subjects. The mean apparent terminal elimination half-lives for R( + )-carvedilol range from 5 to 9 hours compared with 7 to 11 hours for the S( - )-enantiomer.
The primary P450 enzymes responsible for the metabolism of both R(+) and S()-carvedilol in human liver microsomes were CYP2D6 and CYP2C9 and to a lesser extent CYP3A4, 2C19, 1A2, and 2E1. CYP2D6 is thought to be the major enzyme in the 4' and 5'-hydroxylation of carvedilol, with a potential contribution from 3A4. CYP2C9 is thought to be of primary importance in the O-methylation pathway of S(-)-carvedilol.
Carvedilol is subject to the effects of genetic polymorphism with poor metabolizers of debrisoquin (a marker for cytochrome P450 2D6) exhibiting 2- to 3-fold higher plasma concentrations of R( + )-carvedilol compared with extensive metabolizers. In contrast, plasma levels of S( - )-carvedilol are increased only about 20% to 25% in poor metabolizers, indicating this enantiomer is metabolized to a lesser extent by cytochrome P450 2D6 than R( + )-carvedilol. The pharmacokinetics of carvedilol do not appear to be different in poor metabolizers of S-mephenytoin (patients deficient in cytochrome P450 2C19).
Carvedilol is more than 98% bound to plasma proteins, primarily with albumin. The plasma-protein binding is independent of concentration over the therapeutic range. Carvedilol is a basic, lipophilic compound with a steady-state volume of distribution of approximately 115 L, indicating substantial distribution into extravascular tissues. Plasma clearance ranges from 500 to 700 mL/min.
13.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
In 2-year studies conducted in rats given carvedilol at doses up to 75 mg per kg per day (12 times the MRHD as mg per m²) or in mice given up to 200 mg per kg per day (16 times the MRHD as mg per m²), carvedilol had no carcinogenic effect.
Carvedilol was negative when tested in a battery of genotoxicity assays, including the Ames and the CHO/HGPRT assays for mutagenicity and the in vitro hamster micronucleus and in vivo human lymphocyte cell tests for clastogenicity.
In a combined fertility/developmental/post-natal toxicity study, rats were given carvedilol (12, 60, 300 mg per kg per day) orally by gavage for 2 weeks before mating and through mating, gestation, and weaning for females and for 62 days prior to and through mating for males. At a dosage of 300 mg per kg per day (greater than or equal to 50 times the MRHD as mg per m²) carvedilol was toxic to adult rats (sedation, reduced weight gain) and was associated with a reduced number of successful matings, prolonged mating time, fewer corpora lutea and implants per dam, fewer live pups per litter, and delays in physical growth/development. The no-effect level for overt toxicity and impairment of fertility was 60 mg per kg per day (10 times the MRHD as mg per m²).
14. Clinical Studies
14.1 Heart Failure
A total of 6,975 subjects with mild-to-severe heart failure were evaluated in placebo-controlled trials of carvedilol.
Mild-to-Moderate Heart Failure
Carvedilol was studied in 5 multicenter, placebo-controlled trials, and in 1 active-controlled trial (COMET trial) involving subjects with mild-to-moderate heart failure.
Four U.S. multicenter, double-blind, placebo-controlled trials enrolled 1,094 subjects (696 randomized to carvedilol) with NYHA class II to III heart failure and ejection fraction less than or equal to 0.35. The vast majority were on digitalis, diuretics, and an ACE inhibitor at trial entry. Patients were assigned to the trials based upon exercise ability. An Australia-New Zealand double-blind, placebo-controlled trial enrolled 415 subjects (half randomized to carvedilol) with less severe heart failure. All protocols excluded subjects expected to undergo cardiac transplantation during the 7.5 to 15 months of double-blind follow-up. All randomized subjects had tolerated a 2-week course on carvedilol 6.25 mg twice daily.
In each trial, there was a primary end point, either progression of heart failure (1 U.S. trial) or exercise tolerance (2 U.S. trials meeting enrollment goals and the Australia-New Zealand trial). There were many secondary end points specified in these trials, including NYHA classification, patient and physician global assessments, and cardiovascular hospitalization. Other analyses not prospectively planned included the sum of deaths and total cardiovascular hospitalizations. In situations where the primary end points of a trial do not show a significant benefit of treatment, assignment of significance values to the other results is complex, and such values need to be interpreted cautiously.
The results of the U.S. and Australia-New Zealand trials were as follows:
Slowing Progression of Heart Failure: One U.S. multicenter trial (366 subjects) had as its primary end point the sum of cardiovascular mortality, cardiovascular hospitalization, and sustained increase in heart failure medications. Heart failure progression was reduced, during an average follow-up of 7 months, by 48% (P = 0.008).
In the Australia-New Zealand trial, death and total hospitalizations were reduced by about 25% over 18 to 24 months. In the 3 largest U.S. trials, death and total hospitalizations were reduced by 19%, 39%, and 49%, nominally statistically significant in the last 2 trials. The Australia-New Zealand results were statistically borderline.
Functional Measures: None of the multicenter trials had NYHA classification as a primary end point, but all such trials had it as a secondary end point. There was at least a trend toward improvement in NYHA class in all trials. Exercise tolerance was the primary end point in 3 trials; in none was a statistically significant effect found.
Subjective Measures: Health-related quality of life, as measured with a standard questionnaire (a primary end point in 1 trial), was unaffected by carvedilol. However, patients' and investigators' global assessments showed significant improvement in most trials.
Mortality: Death was not a pre-specified end point in any trial, but was analyzed in all trials. Overall, in these 4 U.S. trials, mortality was reduced, nominally significantly so in 2 trials.
The COMET Trial
In this double-blind trial, 3,029 subjects with NYHA class II to IV heart failure (left ventricular ejection fraction less than or equal to 35%) were randomized to receive either carvedilol (target dose: 25 mg twice daily) or immediate-release metoprolol tartrate (target dose: 50 mg twice daily). The mean age of the subjects was approximately 62 years, 80% were males, and the mean left ventricular ejection fraction at baseline was 26%. Approximately 96% of the subjects had NYHA class II or III heart failure. Concomitant treatment included diuretics (99%), ACE inhibitors (91%), digitalis (59%), aldosterone antagonists (11%), and "statin" lipid-lowering agents (21%). The mean duration of follow-up was 4.8 years. The mean dose of carvedilol was 42 mg per day.
The trial had 2 primary end points: all-cause mortality and the composite of death plus hospitalization for any reason. The results of COMET are presented in Table 3 below. All-cause mortality carried most of the statistical weight and was the primary determinant of the trial size. All-cause mortality was 34% in the subjects treated with carvedilol and was 40% in the immediate-release metoprolol group (P = 0.0017; hazard ratio = 0.83, 95% CI: 0.74 to 0.93). The effect on mortality was primarily due to a reduction in cardiovascular death. The difference between the 2 groups with respect to the composite end point was not significant (P = 0.122).
The estimated mean survival was 8 years with carvedilol and 6.6 years with immediate-release metoprolol.
Table 3. Results of COMET:
| End Point | Carvedilol n=1,511 | Metoprolol n=1,518 | Hazard Ratio | (95% CI) |
|---|---|---|---|---|
| All-cause mortality | 34% | 40% | 0.83 | 0.74 – 0.93 |
| Mortality + all hospitalization | 74% | 76% | 0.94 | 0.86 – 1.02 |
| Cardiovascular death | 30% | 35% | 0.8 | 0.7 – 0.9 |
| Sudden death Death due to circulatory failure Death due to stroke | 14% 11% 0.9% | 17% 13% 2.5% | 0.81 0.83 0.33 | 0.68 – 0.97 0.67 – 1.02 0.18 – 0.62 |
It is not known whether this formulation of metoprolol at any dose or this low dose of metoprolol in any formulation has any effect on survival or hospitalization in patients with heart failure.
Thus, this trial extends the time over which carvedilol manifests benefits on survival in heart failure, but it is not evidence that carvedilol improves outcome over the formulation of metoprolol (TOPROL-XL) with benefits in heart failure.
Severe Heart Failure (COPERNICUS)
In a double-blind trial (COPERNICUS), 2,289 subjects with heart failure at rest or with minimal exertion and left ventricular ejection fraction less than 25% (mean 20%), despite digitalis (66%), diuretics (99%), and ACE inhibitors (89%), were randomized to placebo or carvedilol. Carvedilol was titrated from a starting dose of 3.125 mg twice daily to the maximum tolerated dose or up to 25 mg twice daily over a minimum of 6 weeks. Most subjects achieved the target dose of 25 mg. The trial was conducted in Eastern and Western Europe, the United States, Israel, and Canada.
Similar numbers of subjects per group (about 100) withdrew during the titration period.
The primary end point of the trial was all-cause mortality, but cause-specific mortality and the risk of death or hospitalization (total, cardiovascular [CV], or heart failure [HF]) were also examined. The developing trial data were followed by a data monitoring committee, and mortality analyses were adjusted for these multiple looks. The trial was stopped after a median follow-up of 10 months because of an observed 35% reduction in mortality (from 19.7% per patient-year on placebo to 12.8% on carvedilol; hazard ratio 0.65, 95% CI: 0.52 to 0.81, P = 0.0014, adjusted) (see Figure 1). The results of COPERNICUS are shown in Table 4.
Table 4. Results of COPERNICUS Trial in Subjects with Severe Heart Failure:
| End Point | Placebo (n=1,133) | Carvedilol (n=1,156) | Hazard Ratio (95% CI) | % Reduction | Nominal Pvalue |
|---|---|---|---|---|---|
| Mortality | 190 | 130 | 0.65 (0.52 – 0.81) | 35 | 0.00013 |
| Mortality + all hospitalization | 507 | 425 | 0.76 (0.67 – 0.87) | 24 | 0.00004 |
| Mortality + CV hospitalization | 395 | 314 | 0.73 (0.63 – 0.84) | 27 | 0.00002 |
| Mortality + HF hospitalization | 357 | 271 | 0.69 (0.59 – 0.81) | 31 | 0.000004 |
Cardiovascular = CV; Heart failure = HF.
Figure 1. Survival Analysis of COPERNICUS (Intent-to-Treat):
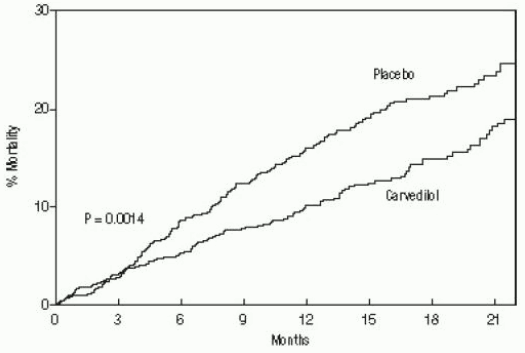
The effect on mortality was principally the result of a reduction in the rate of sudden death among subjects without worsening heart failure.
Patients' global assessments, in which carvedilol-treated subjects were compared with placebo, were based on pre-specified, periodic patient self-assessments regarding whether clinical status post-treatment showed improvement, worsening, or no change compared with baseline. Subjects treated with carvedilol showed significant improvements in global assessments compared with those treated with placebo in COPERNICUS.
The protocol also specified that hospitalizations would be assessed. Fewer subjects on carvedilol than on placebo were hospitalized for any reason (372 versus 432, P = 0.0029), for cardiovascular reasons (246 versus 314, P = 0.0003), or for worsening heart failure (198 versus 268, P= 0.0001).
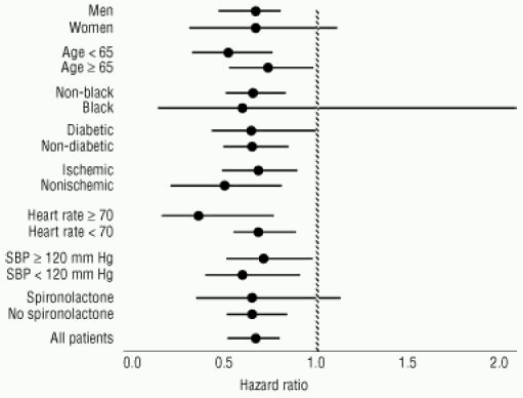
Carvedilol had a consistent and beneficial effect on all-cause mortality as well as the combined end points of all-cause mortality plus hospitalization (total, CV, or for heart failure) in the overall trial population and in all subgroups examined, including men and women, elderly and non-elderly, blacks and non-blacks, and diabetics and non-diabetics (see Figure 2).
Figure 2. Effects of Mortality for Subgroups in COPERNICUS:
14.2 Left Ventricular Dysfunction following Myocardial Infarction
CAPRICORN was a double-blind trial comparing carvedilol and placebo in 1,959 subjects with a recent myocardial infarction (within 21 days) and left ventricular ejection fraction of less than or equal to 40%, with (47%) or without symptoms of heart failure. Subjects given carvedilol received 6.25 mg twice daily, titrated as tolerated to 25 mg twice daily. Subjects had to have a systolic blood pressure greater than 90 mm Hg, a sitting heart rate greater than 60 beats per minute, and no contraindication to β-blocker use. Treatment of the index infarction included aspirin (85%), IV or oral β-blockers (37%), nitrates (73%), heparin (64%), thrombolytics (40%), and acute angioplasty (12%). Background treatment included ACE inhibitors or angiotensin-receptor blockers (97%), anticoagulants (20%), lipid-lowering agents (23%), and diuretics (34%). Baseline population characteristics included an average age of 63 years, 74% male, 95% Caucasian, mean blood pressure 121/74 mm Hg, 22% with diabetes, and 54% with a history of hypertension. Mean dosage achieved of carvedilol was 20 mg twice daily; mean duration of follow-up was 15 months.
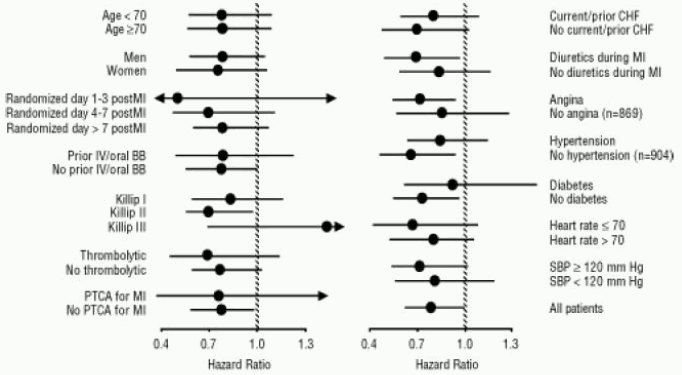
All-cause mortality was 15% in the placebo group and 12% in the carvedilol group, indicating a 23% risk reduction in subjects treated with carvedilol (95% CI: 2% to 40%, P = 0.03), as shown in Figure 3. The effects on mortality in various subgroups are shown in Figure 4. Nearly all deaths were cardiovascular (which were reduced by 25% by carvedilol), and most of these deaths were sudden or related to pump failure (both types of death were reduced by carvedilol). Another trial end point, total mortality and all-cause hospitalization, did not show a significant improvement.
There was also a significant 40% reduction in fatal or non-fatal myocardial infarction observed in the group treated with carvedilol (95% CI: 11% to 60%, P = 0.01). A similar reduction in the risk of myocardial infarction was also observed in a meta-analysis of placebo-controlled trials of carvedilol in heart failure.
Figure 3. Survival Analysis for CAPRICORN (Intent-to-Treat):
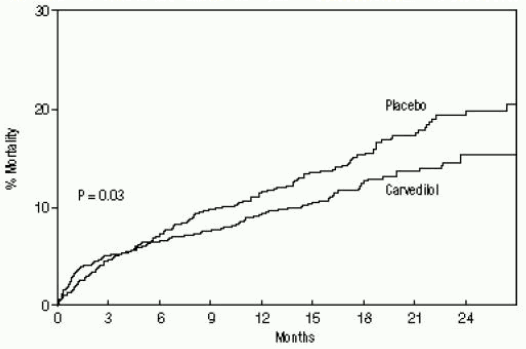
Figure 4. Effects on Mortality for Subgroups in CAPRICORN:
14.3 Hypertension
Carvedilol was studied in 2 placebo-controlled trials that utilized twice-daily dosing at total daily doses of 12.5 to 50 mg. In these and other trials, the starting dose did not exceed 12.5 mg. At 50 mg per day, carvedilol reduced sitting trough (12-hour) blood pressure by about 9/5.5 mm Hg; at 25 mg per day the effect was about 7.5/3.5 mm Hg. Comparisons of trough-to-peak blood pressure showed a trough-to-peak ratio for blood pressure response of about 65%. Heart rate fell by about 7.5 beats per minute at 50 mg per day. In general, as is true for other β-blockers, responses were smaller in black than non-black subjects. There were no age- or gender-related differences in response.
The peak antihypertensive effect occurred 1 to 2 hours after a dose. The dose-related blood pressure response was accompanied by a dose-related increase in adverse effects [see Adverse Reactions (6)].
14.4 Hypertension with Type 2 Diabetes Mellitus
In a double-blind trial (GEMINI), carvedilol, added to an ACE inhibitor or angiotensin-receptor blocker, was evaluated in a population with mild-to-moderate hypertension and well-controlled type 2 diabetes mellitus. The mean HbA1c at baseline was 7.2%. Carvedilol was titrated to a mean dose of 17.5 mg twice daily and maintained for 5 months. Carvedilol had no adverse effect on glycemic control, based on HbA1c measurements (mean change from baseline of 0.02%, 95% CI: -0.06 to 0.1, P= NS) [see Warnings and Precautions (5.6)].
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.