MEDRONE Tablet Ref.[7316] Active ingredients: Methylprednisolone
Source: Medicines & Healthcare Products Regulatory Agency (GB) Revision Year: 2019 Publisher: Pfizer Ltd, Ramsgate Road, Sandwich, Kent, CT13 9NJ, UK
Contraindications
Methylprednisolone tablets are contraindicated:
- In patients who have systemic fungal infections.
- In patients who have systemic infections unless specific anti-infective therapy is employed.
- In patients who have hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
Administration of live or live, attenuated vaccines is contraindicated in patients receiving immunosuppressive doses of corticosteroids.
Special warnings and precautions for use
Immunosuppressant Effects/Increased Susceptibility to Infections
Corticosteroids may increase susceptibility to infection, may mask some signs of infection, and new infections may appear during their use. Suppression of the inflammatory response and immune function increases the susceptibility to fungal, viral and bacterial infections and their severity. The clinical presentation may often be atypical and may reach an advanced stage before being recognised.
Persons who are on drugs which suppress the immune system are more susceptible to infections than healthy individuals. Chicken pox and measles, for example, can have a more serious or even fatal course in non-immune children or adults on corticosteroids.
Chickenpox is of serious concern since this normally minor illness may be fatal in immunosuppressed patients. Patients (or parents of children) without a definite history of chickenpox should be advised to avoid close personal contact with chickenpox or herpes zoster and if exposed they should seek urgent medical attention. Passive immunization with varicella/zoster immunoglobulin (VZIG) is needed by exposed non-immune patients who are receiving systemic corticosteroids or who have used them within the previous 3 months; this should be given within 10 days of exposure to chickenpox. If a diagnosis of chickenpox is confirmed, the illness warrants specialist care and urgent treatment. Corticosteroids should not be stopped and the dose may need to be increased.
Exposure to measles should be avoided. Medical advice must be sought immediately if exposure occurs. Prophylaxis with normal intramuscular immunoglobulin may be needed.
Similarly corticosteroids should be used with great care in patients with known or suspected parasitic infections such as Strongyloides (threadworm) infestation, which may lead to Strongyloides hyperinfection and dissemination with widespread larval migration, often accompanied by severe enterocolitis and potentially fatal gram-negative septicemia.
Administration of live or live, attenuated vaccines is contraindicated in patients receiving immunosuppressive doses of corticosteroids. The antibody response to other vaccines may be diminished.
The use of corticosteroids in active tuberculosis should be restricted to those cases of fulminating or disseminated tuberculosis in which the corticosteroid is used for the management of the disease in conjunction with an appropriate antituberculous regimen. If corticosteroids are indicated in patients with latent tuberculosis or tuberculin reactivity, close observation is necessary as reactivation of the disease may occur. During prolonged corticosteroid therapy, these patients should receive chemoprophylaxis.
Kaposi’s sarcoma has been reported to occur in patients receiving corticosteroid therapy. Discontinuation of corticosteroids may result in clinical remission.
The role of corticosteroids in septic shock has been controversial, with early studies reporting both beneficial and detrimental effects. More recently, supplemental corticosteroids have been suggested to be beneficial in patients with established septic shock who exhibit adrenal insufficiency. However, their routine use in septic shock is not recommended. A systematic review of short-course high-dose corticosteroids did not support their use. However, meta-analyses, and a review have suggested that longer courses (5-11 days) of low-dose corticosteroids might reduce mortality.
Immune System
Because rare instances of skin reactions and anaphylactic/anaphylactoid reactions have occurred in patients receiving corticosteroid therapy, appropriate precautionary measures should be taken prior to administration, especially when the patient has a history of allergy to any drug.
Endocrine Effects
In patients on corticosteroid therapy subjected to unusual stress, increased dosage of rapidly acting corticosteroids before, during, and after the stressful situation is indicated.
Adrenal cortical atrophy develops during prolonged therapy and may persist for months after stopping treatment. In patients who have received more than physiological doses of systemic corticosteroids (approximately 6 mg methylprednisolone) for greater than 3 weeks, withdrawal should not be abrupt. How dose reduction should be carried out depends largely on whether the disease is likely to relapse as the dose of systemic corticosteroids is reduced. Clinical assessment of disease activity may be needed during withdrawal. If the disease is unlikely to relapse on withdrawal of systemic corticosteroids, but there is uncertainty about HPA suppression, the dose of systemic corticosteroid may be reduced rapidly to physiological doses. Once a daily dose of 6 mg methylprednisolone is reached, dose reduction should be slower to allow the HPA-axis to recover.
Abrupt withdrawal of systemic corticosteroid treatment, which has continued up to 3 weeks is appropriate if it considered that the disease is unlikely to relapse. Abrupt withdrawal of doses up to 32 mg daily of methylprednisolone for 3 weeks is unlikely to lead to clinically relevant HPA-axis suppression, in the majority of patients. In the following patient groups, gradual withdrawal of systemic corticosteroid therapy should be considered even after courses lasting 3 weeks or less:
- Patients who have had repeated courses of systemic corticosteroids, particularly if taken for greater than 3 weeks.
- When a short course has been prescribed within one year of cessation of long-term therapy (months or years).
- Patients who may have reasons for adrenocortical insufficiency other than exogenous corticosteroid therapy. In addition, acute adrenal insufficiency leading to a fatal outcome may occur if glucocorticoids are withdrawn abruptly.
- Patients receiving doses of systemic corticosteroid greater than 32 mg daily of methylprednisolone.
- Patients repeatedly taking doses in the evening.
A steroid “withdrawal syndrome,” seemingly unrelated to adrenocortical insufficiency, may also occur following abrupt discontinuance of glucocorticoids. This syndrome includes symptoms such as: anorexia, nausea, vomiting, lethargy, headache, fever, joint pain, desquamation, myalgia, weight loss, and/or hypotension. These effects are thought to be due to the sudden change in glucocorticoid concentration rather than to low corticosteroid levels.
Glucocorticoids can produce or aggravate Cushing’s syndrome, therefore glucocorticoids should be avoided in patients with Cushing’s disease.
Particular care is required when considering the use of systemic corticosteroids in patients with hypothyroidism and frequent patient monitoring is necessary.
Metabolism and Nutrition Disorders
Corticosteroids, including methylprednisolone, can increase blood glucose, worsen pre-existing diabetes, and predispose those on long-term corticosteroid therapy to diabetes mellitus.
Particular care is required when considering the use of systemic corticosteroids in patients with Diabetes mellitus (or a family history of diabetes) and frequent patient monitoring is necessary.
Psychiatric Effects
Patients and/or carers should be warned that potentially severe psychiatric adverse reactions may occur with systemic steroids (see section 4.8). Symptoms typically emerge within a few days or weeks of starting treatment. Risks may be higher with high doses/systemic exposure (see also section 4.5), although dose levels do not allow prediction of the onset, type, severity or duration of reactions. Most reactions recover after either dose reduction or withdrawal, although specific treatment may be necessary.
Patients/carers should be encouraged to seek medical advice if worrying psychological symptoms develop, especially if depressed mood or suicidal ideation is suspected. Patients/carers should be alert to possible psychiatric disturbances that may occur either during or immediately after dose tapering/withdrawal of systemic steroids, although such reactions have been reported infrequently.
Particular care is required when considering the use of systemic corticosteroids in patients with existing or previous history of severe affective disorders in themselves or in their first degree relatives. These would include depressive or manic-depressive illness and previous steroid psychosis.
Nervous System Effects
Particular care is required when considering the use of systemic corticosteroids in patients with seizure disorders and myasthenia gravis (see myopathy statement in Musculoskeletal Effects section) and frequent patient monitoring is necessary.
There have been reports of epidural lipomatosis in patients taking corticosteroids, typically with long-term use at high doses.
Ocular Effects
Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids. Central serous chorioretinopathy, may lead to retinal detachment.
Particular care is required when considering the use of systemic corticosteroids in patients with glaucoma (or a family history of glaucoma) and ocular herpes simplex as there is a fear of corneal perforation, and frequent patient monitoring is necessary.
Prolonged use of corticosteroids may produce posterior subcapsular cataracts and nuclear cataracts (particularly in children), exophthalmos or increased intraocular pressure, which may result in glaucoma with possible damage to the optic nerves.
Secondary fungal and viral infections of the eye may also be enhanced in patients receiving glucocorticoids.
Cardiac Events
Adverse effects of glucocorticoids on the cardiovascular system, such as dyslipidemia and hypertension, may predispose treated patients with existing cardiovascular risk factors to additional cardiovascular effects, if high doses and prolonged courses are used. Accordingly, corticosteroids should be employed judiciously in such patients and attention should be paid to risk modification and additional cardiac monitoring if needed. Low dose and alternate day therapy may reduce the incidence of complications in corticosteroid therapy.
Systemic corticosteroids should be used with caution, and only if strictly necessary, in cases of congestive heart failure.
Particular care is required when considering the use of systemic corticosteroids in patients with recent myocardial infarction (myocardial rupture has been reported) and frequent patient monitoring is necessary.
Care should be taken for patients receiving cardioactive drugs such as digoxin because of steroid induced electrolyte disturbance/potassium loss (see section 4.8).
Vascular Effects
Particular care is required when considering the use of systemic corticosteroids in patients with the following conditions and frequent patient monitoring is necessary.
Hypertension
Predisposition to thrombophlebitis
Thrombosis including venous thromboembolism has been reported to occur with corticosteroids. As a result corticosteroids should be used with caution in patients who have or may be predisposed to thromboembolic disorders.
Gastrointestinal Effects
High doses of corticosteroids may produce acute pancreatitis.
Particular care is required when considering the use of systemic corticosteroids in patients with the following conditions and frequent patient monitoring is necessary.
Peptic ulceration.
Fresh intestinal anastomoses.
Abscess or other pyogenic infections.
Ulcerative colitis.
Diverticulitis.
Glucocorticoid therapy may mask peritonitis or other signs or symptoms associated with gastrointestinal disorders such as perforation, obstruction or pancreatitis. In combination with NSAIDs, the risk of developing gastrointestinal ulcers is increased.
Hepatobiliary Effects
Particular care is required when considering the use of systemic corticosteroids in patients with liver failure or cirrhosis and frequent patient monitoring is necessary.
Rarely hepatobiliary disorders were reported, in the majority of these cases, they were reversible after withdrawal of therapy. Therefore appropriate monitoring is required.
Musculoskeletal Effects
An acute myopathy has been reported with the use of high doses of corticosteroids, most often occurring in patients with disorders of neuromuscular transmission (e.g. myasthenia gravis), or in patients receiving concomitant therapy with anticholinergics, such as neuromuscular blocking drugs (e.g. pancuronium). This acute myopathy is generalized, may involve ocular and respiratory muscles, and may result in quadriparesis. Elevations of creatine kinase may occur. Clinical improvement or recovery after stopping corticosteroids may require weeks to years.
Particular care is required when considering the use of systemic corticosteroids in patients with osteoporosis (post-menopausal females are particularly at risk) and frequent patient monitoring is necessary.
Renal and Urinary
Caution is required in patients with systemic sclerosis because an increased incidence of scleroderma renal crisis has been observed with corticosteroids, including methylprednisolone. Blood pressure and renal function (s-creatinine) should therefore be routinely checked. When renal crisis is suspected, blood pressure should be carefully controlled.
Particular care is required when considering the use of systemic corticosteroids in patients with renal insufficiency and frequent patient monitoring is necessary.
Injury, poisoning and procedural complications
Systemic corticosteroids are not indicated for, and therefore should not be used to treat, traumatic brain injury, a multicenter study revealed an increased mortality at 2 weeks and 6 months after injury in patients administered methylprednisolone sodium succinate compared to placebo. A causal association with methylprednisolone sodium succinate treatment has not been established.
Other
Undesirable effects may be minimised by using the lowest effective dose for the minimum period, and by administering the daily requirement as a single morning dose or whenever possible as a single morning dose on alternative days. Frequent patient review is required to appropriately titrate the dose against disease activity (see section 4.2).
Patients should carry ‘Steroid Treatment’ cards which give clear guidance on the precautions to be taken to minimise risk and which provide details of prescriber, drug, dosage and the duration of treatment.
Co-treatment with CYP3A inhibitors, including cobicistat-containing products, is expected to increase the risk of systemic side-effects. The combination should be avoided unless the benefit outweighs the increased risk of systemic corticosteroid side-effects, in which case patients should be monitored for systemic corticosteroid side-effects (see section 4.5).
Aspirin and non-steroidal anti-inflammatory agents should be used cautiously in conjunction with corticosteroids.
Pheochromocytoma crisis, which can be fatal, has been reported after administration of systemic corticosteroids. Corticosteroids should only be administered to patients with suspected or identified pheochromocytoma after an appropriate risk/benefit evaluation.
Paediatric population
Corticosteroids cause growth retardation in infancy, childhood and adolescence. Growth and development of infants and children on prolonged corticosteroid therapy should be carefully observed. Treatment should be limited to the minimum dosage for the shortest possible time. In order to minimise suppression of the hypothalamo-pituitary-adrenal axis and growth retardation, treatment should be administered where possible as a single dose on alternate days (see section 4.2).
Infants and children on prolonged corticosteroid therapy are at special risk from raised intracranial pressure.
High doses of corticosteroids may produce pancreatitis in children.
Use in the elderly: The common adverse effects of systemic corticosteroids may be associated with more serious consequences in old age, especially osteoporosis, hypertension, hypokalaemia, diabetes, susceptibility to infection and thinning of the skin. Close clinical supervision is required to avoid life-threatening reactions.
Ingredient warning
This medicine contains lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
This medicine contains sucrose. Patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take this medicine.
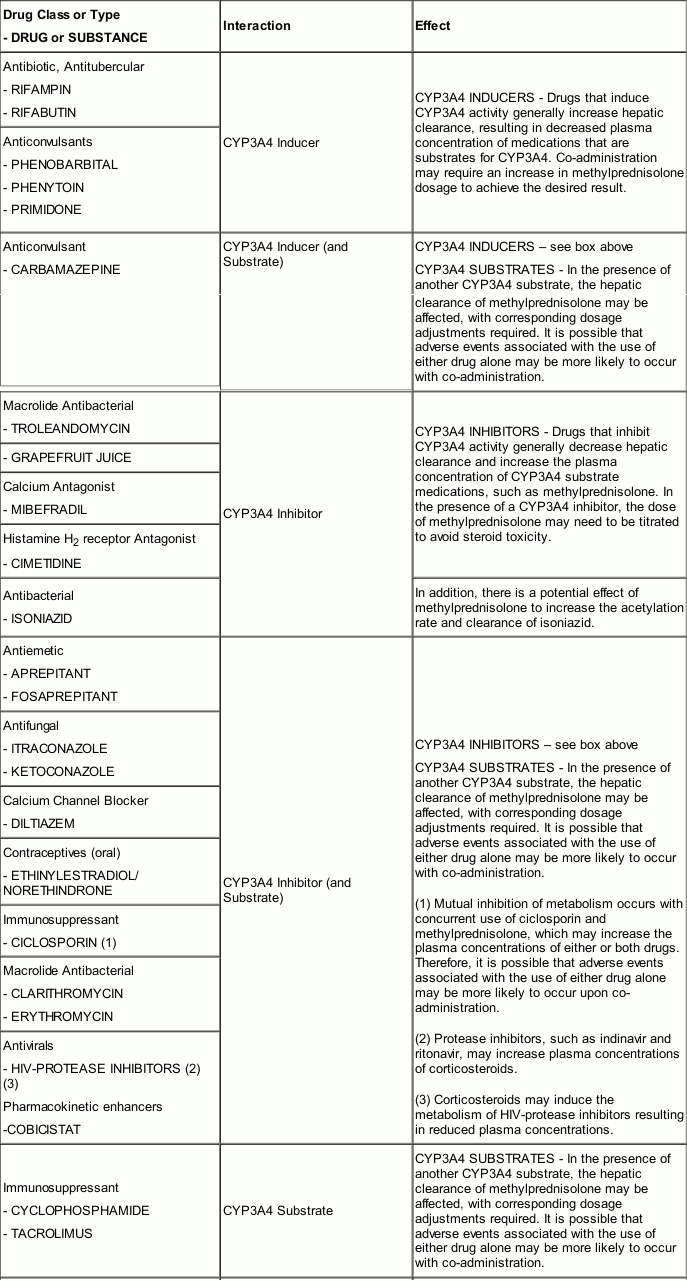
Interaction with other medicinal products and other forms of interaction
Methylprednisolone is a cytochrome P450 enzyme (CYP) substrate and is mainly metabolized by the CYP3A4 enzyme. CYP3A4 is the dominant enzyme of the most abundant CYP subfamily in the liver of adult humans. It catalyzes 6β-hydroxylation of steroids, the essential Phase I metabolic step for both endogenous and synthetic corticosteroids. Many other compounds are also substrates of CYP3A4, some of which (as well as other drugs) have been shown to alter glucocorticoid metabolism by induction (upregulation) or inhibition of the CYP3A4 enzyme.

Fertility, pregnancy and lactation
Fertility
Corticosteroids have been shown to impair fertility in animal studies (see section 5.3).
Pregnancy
The ability of corticosteroids to cross the placenta varies between individual drugs, however, methylprednisolone does cross the placenta. In humans, the risk of low birth weight appears to be dose related and may be minimized by administering lower corticosteroid doses.
Administration of corticosteroids to pregnant animals can cause abnormalities of foetal development including cleft palate, intra-uterine growth retardation and effects on brain growth and development. There is no evidence that corticosteroids result in an increased incidence of congenital abnormalities, such as cleft palate in man, however, when administered for long periods or repeatedly during pregnancy, corticosteroids may increase the risk of intra-uterine growth retardation. Infants born to mothers, who have received substantial doses of corticosteroids during pregnancy must be carefully observed and evaluated for signs of adrenal insufficiency. Hypoadrenalism may, in theory, occur in the neonate following prenatal exposure to corticosteroids but usually resolves spontaneously following birth and is rarely clinically important.
Since adequate human reproductive studies have not been done with methylprednisolone, this medicinal product, as with all drugs, should be used during pregnancy only after a careful assessment of the benefit-risk ratio to the mother, embryo, foetus or child. When corticosteroids are essential, however, patients with normal pregnancies may be treated as though they were in the non-gravid state.
Cataracts have been observed in infants born to mothers undergoing long-term treatment with corticosteroids during pregnancy.
Breast-feeding
Corticosteroids are excreted in small amounts in breast milk, however, doses of up to 40 mg daily of methylprednisolone are unlikely to cause systemic effects in the infant. Infants of mothers taking higher doses than this may have a degree of adrenal suppression. This medicinal product should be used during breast feeding only after a careful assessment of the benefit-risk ratio to the mother and infant.
Effects on ability to drive and use machines
The effect of corticosteroids on the ability to drive or use machinery has not been systematically evaluated. Undesirable effects, such as dizziness, vertigo, visual disturbances and fatigue are possible after treatment with corticosteroids. If affected, patients should not drive or operate machinery.
Undesirable effects
Infections and infestations
Common: Infection (including increased susceptibility and severity of infections with suppression of clinical symptoms and signs)
Not Known: Opportunistic infection; recurrence of dormant tuberculosis, Peritonitis†
Blood and lymphatic system disorders
Not Known: Leukocytosis
Immune system disorders
Not Known: Drug hypersensitivity, Anaphylactic reaction, Anaphylactoid reaction
Endocrine disorders
Common: Cushingoid
Not Known: Hypopituitarism
Neoplasms benign, malignant and unspecified (including cysts and polyps)
Not Known: Kaposi’s sarcoma
Metabolism and nutrition disorders
Common: Sodium retention; Fluid retention
Not Known: Metabolic acidosis; Alkalosis hypokalaemic; Dyslipidaemia; Glucose tolerance impaired; increased requirements for insulin (or oral hypoglycemic agents in diabetics); Lipomatosis; Increased appetite (which may result in Weight increased); Epidural lipomatosis
Psychiatric disorders
Common: Affective disorder (including Depressed mood and Euphoric mood)
Not Known: Psychotic disorder (including Mania, Delusion, Hallucination, and Schizophrenia; Psychotic behaviour; Affective disorder (including Affect lability, Psychological dependence, Suicidal ideation); Mental disorder; Personality change; Confusional state; Anxiety; Mood swings; Abnormal behaviour; Insomnia; Irritability
Nervous system disorders
Not Known: Intracranial pressure increased (with Papilloedema [Benign intracranial hypertension]); Seizure; Amnesia; Cognitive disorder; Dizziness; Headache
Eye disorders
Common: Cataract
Rare: Vision blurred (see also section 4.4)
Not Known: Glaucoma; Exophthalmos; Corneal thinning; Scleral thinning; Chorioretinopathy
Ear and labyrinth disorders
Not Known: Vertigo
Cardiac disorders
Not Known: Cardiac failure congestive (in susceptible patients); Myocardial rupture following myocardial infarction
Vascular disorders
Common: Hypertension
Not Known: Hypotension; Embolism arterial; Thrombotic events
Respiratory, thoracic and mediastinal disorders
Not Known: Pulmonary embolism, Hiccups
Gastrointestinal disorders
Common: Peptic ulcer (with possible Peptic ulcer perforation and Peptic ulcer haemorrhage)
Not Known: Intestinal perforation; Gastric haemorrhage; Pancreatitis; Oesophagitis ulcerative; Oesophagitis; Abdominal distension; Abdominal pain; Diarrhoea; Dyspepsia; Nausea
Hepatobiliary disorders
Not Known: Increase of liver enzymes (e.g. alanine aminotransferase increased, aspartate aminotransferase increased)
Skin and subcutaneous tissue disorders
Common: Skin atrophy; Acne
Not Known: Angioedema; Hirsutism; Petechiae; Ecchymosis; Erythema; Hyperhidrosis; Skin striae; Rash; Pruritus; Urticaria; Telangiectasia
Musculoskeletal and connective tissue disorders
Common: Muscular weakness; Growth retardation
Not Known: Myalgia; Myopathy; Muscle atrophy; Osteoporosis; Osteonecrosis; Pathologic fracture; Neuropathic arthropathy; Arthralgia;
Reproductive system and breast disorders
Not Known: Menstruation irregular
General disorders and administration site conditions
Common: Impaired healing
Not Known: Oedema peripheral ;Fatigue; Malaise; Withdrawal symptoms – too rapid a reduction of corticosteroid dosage following prolonged treatment can lead to acute adrenal insufficiency, hypotension and death (see section 4.4)
Investigations
Common: Blood potassium decreased
Not Known: Intraocular pressure increased; Carbohydrate tolerance decreased; Urine calcium increased Blood alkaline phosphatase increased; Blood urea increased; Suppression of reactions to skin tests*
Injury, poisoning and procedural complications
Not Known: Tendon rupture (particularly of the Achilles tendon); Spinal compression fracture
* Not a MedDRA PT
† Peritonitis may be the primary presenting sign or symptom of a gastrointestinal disorder such as perforation, obstruction or pancreatitis (see section 4.4).
Common (≥1/100 to <1/10); Uncommon (≥1/1,000 to <1/100); Rare (≥1/10,000 to <1/1,000); Not known (frequency cannot be estimated from the available data)
The incidence of predictable undesirable side-effects associated with the use of corticosteroids, including hypothalamic-pituitary-adrenal suppression correlates with the relative potency of the drug, dosage, timing of administration and duration of treatment (see section 4.4).
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the Yellow Card Scheme at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store.
Incompatibilities
Not applicable.
© All content on this website, including data entry, data processing, decision support tools, "RxReasoner" logo and graphics, is the intellectual property of RxReasoner and is protected by copyright laws. Unauthorized reproduction or distribution of any part of this content without explicit written permission from RxReasoner is strictly prohibited. Any third-party content used on this site is acknowledged and utilized under fair use principles.